What is a Head injury?
Definition:
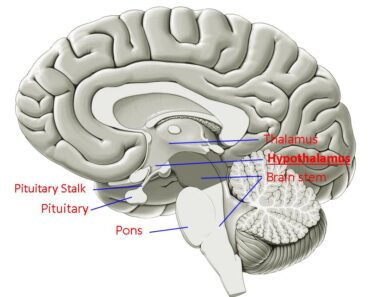
The term ‘Head injury’ is a Neurological Problem or disorder. Its commonly used to describe injuries affecting not just the brain but also the scalp, skull, maxilla, and mandible. and special senses of smell, vision, and hearing. Head injury or craniocerebral trauma/head trauma are used to denote injury to the skull or brain or both that is of sufficient magnitude to interfere with normal function Head injuries are also commonly referred to as brain injury or traumatic brain injury, depending on the extent of the head trauma.
Causes of head injury:
- Head trauma: often causes intracranial bleeding. The common sites are temporal and inferior frontal lobes and into the subarachnoid, subdural, and epidural spaces involved in head trauma Gunshot wound of the brain. Falls (also Road traffic accidents). Blows on the chin (“punch-drunk”), falling objects.
- Hypertensive hemorrhage: results from spontaneous rupture of a small penetrating artery deep in the brain.
- Metastatic brain tumor: Choriocarcinoma, malignant melanoma, renal cell carcinoma, and bronchogenic carcinoma are the most common metastatic tumors associated with intracerebral hemorrhage. Glioblastoma in adults and medulloblastoma in children.
- Dural arteriovenous fistula: Depending on the magnitude of the shunt, venous pressures may rise high enough to cause cortical ischemia or venous hypertension and hemorrhage.
- Capillary Telangiectasias/ Osler-Rendu-Weber syndrome: These capillary malformations can be seen in patients with hereditary hemorrhagic telangiectasia.
- Transformation of prior ischemic infarction
- Arteriovenous malformation
- Aneurysm, Coagulopathy
- Drug (cocaine)
Classification of Brain injury based on its criteria:
Diffuse Brain injury:
Concussion: Concussion, meaning a reversible traumatic paralysis of the nervous (unction is always immediate (not delayed even by seconds),
Diffuse axonal injury: Another type of deep white matter lesion consists of widespread acute disruption or shearing of axons at the time of impact. Most characteristics are small areas of tissue disruption in the corpus callosum and dorsolateral pons The presence of widespread 3xonal damage of both hemispheres, a state called diffuse axonal injury, explains persistent coma and the vegetative state, but small ischemic-hemorrhagic lesions in the midbrain and thalamus are as often the cause
Focal injury
Focal injuries include contusions, laceration, and intracerebral hemorrhage The frontal-temporal regions are most sensitive to stress injuries. Less common sites of injury are the inferio-lateral angles of the occipital lobes, the medial surfaces of the hemispheres, and the corpus callosum.
a. Contusion
A surface bruise of the brain, or contusion, consists of varying degrees of petechial hemorrhage, edema, and tissue destruction. Contusions and deeper hemorrhages result from mechanical forces that displace the hemispheres forcefully relative to the skull by deceleration of the brain against the inner skull, either under a point of impact (coup lesion) or, as the brain swings back, in the antipolar area (contrecoup lesion.
b. Laceration:
Lacerations are the actual tearing of the cortical surface. Often occurs in association with depressed and compound fractures and penetrating injury. Tissue damage is severe, and surgical repair of the laceration is impossible because of the texture of the brain tissue. If bleeding is deep into the parenchyma, focal & generalized signs are noted.
c. Hemorrhage
Torsion or shearing forces in the brain can cause basal ganglia and other deep hematomas independent of surface damage. Sudden neurologic deterioration in a comatose patient or a sudden rise in intracranial pressure (ICP) should. therefore prompt investigation with a CT scan.
i. Subdural hematoma:
Hemorrhages beneath the dura (subdural) may be associated with contusions and other injuries, making it difficult to determine their relative contribution to the clinical state. However, subdural often occur as the sole manifestation of injury, and each has characteristic clinical and radiologic features. Because the mass effect and the rise in ICP caused by these hemorrhages may be life-threatening.
ii. Epidural hemorrhage:
This arises with a temporal or parietal fracture and laceration of the middle meningeal artery or vein. Less often, there is a tear in a dural venous sinus. Most patients are unconscious when first seen A “lucid interval” of several minutes to hours before coma supervenes is most characteristic of epidural hemorrhage, but it is still uncommon, and epidural hemorrhage by no means is the only cause of this temporal sequence of events.
iii. Intracerebral hemorrhage:
Parenchymal hemorrhage is the most common type of intracranial hemorrhage The most common sites are the basal ganglia (putamen, thalamus, and adjacent deep white matter) deep cerebellum, and pons. In milder cases, edema In adjacent brain tissue may cause progressive deterioration over 12 to 72 h
Thalamic hemorrhages also produce contralateral hemiplegia or hemiparesis from pressure on or dissection into, the adjacent internal capsule.
Cerebellar Hemorrhages usually develop over several hours and are characterized by occipital headache, repeated vomiting, and ataxia of gait. in mild cases, there may be no other neurologic signs other than gait ataxia.
perimesencephalic cisterns and are benign, they probably have a venous capillary source, and angiography is revealing.
Classification of Head injury Based on GCS
Mild brain injury (13-15): GCS score of 13-15 with a loss of consciousness that lasts up to l5mintes. Patients with mild injury often are seen in the emergency department and discharged home.
Moderate brain Injury (9-12): GCS score of 9-12 with a loss of consciousness for up to 6hrs. They ate usually hospitalized. These patients are at risk of cerebral edema & increased intracranial pressure.
Severe brain injury(<8): Patients with a GCS of 8 or less after resuscitation or those who deteriorate to that level within 48 hrs of admission have a severe head injury. In the treatment of head injury these patients need ventilator support and they are placed In critical care settings for monitoring and management.
References:
- https://en.wikipedia.org/wiki/Head_injury
- Elbaum J (2007-04-13). Counseling Individuals Post Acquired Brain Injury. Acquired Brain Injury. Springer New York. pp. 259–274. ISBN 9780387375748.
- Proskuriakova NA, Kasendeeva MK (September 1975). “[Importance of Co35 in the treatment of secondary hypochromic anemia in young children]”. Zdravookhranenie Kirgizii (5): 44–8. PMID 1942.
- Daisley A, Kischka U, Tams R (2008). Head Injury. Oxford: OUP Oxford. ISBN 9780191578717.
- Macfarlane R, Hardy DG (1997). Outcome after Head, Neck and Spinal Trauma: a medicolegal guide. Oxford: Reed Educational and Professional Publishing Ltd. ISBN 978-0-7506-2178-6.