Nursing care plans are a critical part of any nursing process. They provide an organized, systematic approach to patient care and serve as the basis for individualizing patient care. Nursing care plans incorporate assessment data, diagnosis, outcomes, interventions, and evaluation into a comprehensive plan of care. If you are working as a nurse, it is important to understand how to decide on a nursing care plan and how to choose the correct one. Here in this article, we will help you to understand what is NCP nursing care plan with free examples and the format of nursing care plans. The nursing Care Plan PDF File is available here
How to choose a perfect nursing care plan?
A perfect nursing care plan is a plan with the right information and tools to provide the best possible care for a patient. It should include assessment data, diagnosis, outcome goals, interventions, and evaluation of progress. When creating a nursing care plan it is important to remember that the patient comes first. This means you must consider their medical history, medications they take, lifestyle choices, and any other factors related to the patient’s health and well-being.
Follow the below-mentioned steps while preparing a nursing care plan:
Preparing a nursing care plan is important to make sure that the care provided is tailored to meet the patient’s needs. For this reason, it’s important to follow these steps:
- Assess the patient’s condition and collect relevant data.
- Identify nursing diagnoses based on assessment data.
- Develop outcome goals to be achieved by the care plan interventions.
- Choose appropriate interventions that are aimed at achieving the desired outcomes for the patient
The format of nursing care plans
There are different formats for nursing care plans available. Generally, a nursing care plan consists of the following:
- Introduction – This section includes the patient’s name and information about their age, gender, diagnosis, etc.
- Critical Thinking Questions – These questions help nurses think critically when assessing a patient’s condition.
- Nursing Diagnosis – This is a statement of the patient’s condition.
- Outcome Goals – These are goals that the nursing care plan is aimed at achieving.
- Interventions – These include treatments and therapies that are used to achieve the desired outcome.
- Evaluation – This section includes information about how the patient responded.
- Precautions – This section includes information about any precautions that should be taken when providing care to the patient.
Below give a format for Nursing care plans
Formats of different medical conditions for nursing care plans are placed below and are free of cost. You can refer to these formats for future reference:-
Nursing care elements for a fever patient-
- Patient assessment: This includes information about the patient’s temperature, vital signs, symptoms, and any relevant laboratory or diagnostic test results.
- Nursing diagnosis: This is a statement that identifies the specific problem or issue that the patient is facing, such as impaired comfort related to fever and other symptoms.
- Goals and outcomes: These are specific, measurable objectives that the care plan aims to achieve, such as reducing the patient’s temperature to within normal range, relieving discomfort and other symptoms, and identifying and treating the underlying cause of the fever.
- Interventions: These are the actions that will be taken to address the problem or issue identified in the nursing diagnosis. Some interventions may include: -Measuring and recording the patient’s temperature, vital signs, and symptoms -Administering medications as ordered (such as antipyretics, pain relievers, antibiotics) -Monitoring for signs and symptoms of complications -Encouraging the patient to rest and drink fluids -Teaching the patient and family about the importance of reporting any changes in symptoms
- Evaluation: This section includes a plan for monitoring the patient’s progress and determining whether the interventions have been successful.
- Patient education: This includes information that the patient and family need to know to support self-care and to prevent the problem from recurring, such as the importance of hand hygiene, fever management, and the potential complication of the fever.
- Timeframe: A clear indication of when the care plan will be reviewed and updated.
It is important to note that the nursing care plan format may vary depending on the institution or organization, and the care plan should be tailored to the individual patient’s needs and circumstances.
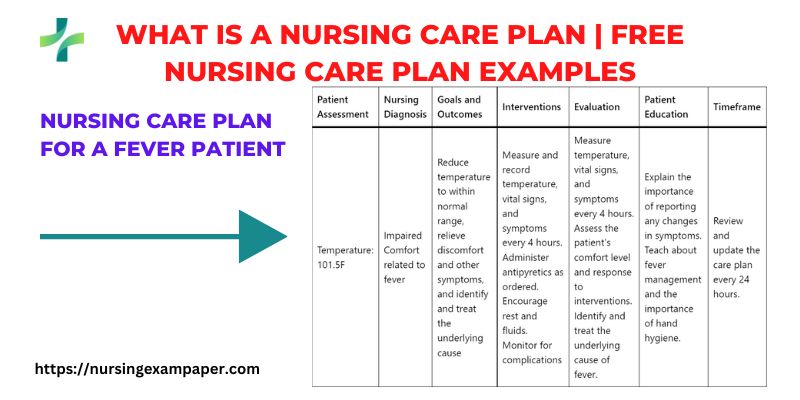
Nursing care plan for a fever patient
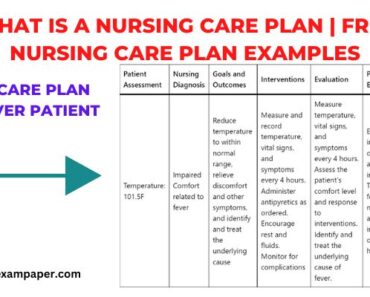
Here is an example of a nursing care plan table format for a patient with a fever:
| Patient Assessment | Nursing Diagnosis | Goals and Outcomes | Interventions | Evaluation | Patient Education | Timeframe |
| Temperature: 101.5F | Impaired Comfort related to fever | Reduce temperature to within normal range, relieve discomfort and other symptoms, and identify and treat the underlying cause | Measure and record temperature, vital signs, and symptoms every 4 hours. Administer antipyretics as ordered. Encourage rest and fluids. Monitor for complications | Measure temperature, vital signs, and symptoms every 4 hours. Assess the patient’s comfort level and response to interventions. Identify and treat the underlying cause of fever. | Explain the importance of reporting any changes in symptoms. Teach about fever management and the importance of hand hygiene. | Review and update the care plan every 24 hours. |
Post-operative nursing care plan
nursing care plan table format for a post-operative patient:
| Patient Assessment | Nursing Diagnosis | Goals and Outcomes | Interventions | Evaluation | Patient Education | Timeframe |
| Vital signs: BP 120/80 mmHg, HR 80 bpm, RR 16/min, T 37.5C | Acute pain related to surgical incision | Reduce pain to a manageable level, promote patient comfort and mobility | Assess pain using a pain scale, and administer pain medication as ordered. Encourage deep breathing and coughing exercises. Position the patient to promote comfort and prevent complications | Assess pain levels and response to interventions. Monitor for signs of infection or bleeding. Document the patient’s mobility and comfort level | Explain the importance of reporting pain and discomfort. Teach pain management techniques and exercises. | Review and update the care plan every 8 hours. |
Nursing care plan for patients with pain
Here is a nursing care plan for patients with pain in table format:
| NURSING CARE PLAN | GOAL/OBJECTIVE | INTERVENTION/NURSING ACTION | EVALUATION |
|---|---|---|---|
| Assessment | Identify and assess the patient’s pain level and location | Use an appropriate pain assessment tool at regular intervals and document the results. Assess any contributing factors to the pain such as medical history, medications, and lifestyle factors. | Observe and document pain level, location, duration, and any contributing factors. |
| Management | Reduce or eliminate the patient’s pain | Implement a pain management plan that includes a combination of non-pharmacological and pharmacological interventions as appropriate. | Monitor the patient’s pain level, and response to interventions, and any side effects. Provide feedback to the healthcare provider as needed. |
| Evaluation | Assess the effectiveness of the pain management plan | Evaluate the patient’s response to pain management interventions using appropriate pain assessment tools. | Assess the patient’s pain level and response to interventions, and any side effects at regular intervals and document the results. |
This nursing care plan includes detailed steps for assessing, managing, and evaluating the patient’s pain. It emphasizes the importance of using appropriate pain assessment tools, identifying contributing factors, implementing a comprehensive pain management plan, and monitoring the patient’s response to interventions.
fracture nursing care plan/nursing diagnosis
Nursing care plan for patients with a fracture.
| NURSING CARE PLAN | GOAL/OBJECTIVE | INTERVENTION/NURSING ACTION | EVALUATION |
|---|---|---|---|
| Assessment | Assess the extent of the fracture and related symptoms | Obtain a thorough history and physical examination of the fracture site, including radiographic imaging as ordered. Assess for any other related injuries or conditions. Identify any factors that may affect healing such as the patient’s age, and overall health status, and adherence to the treatment plan. | Assess and document the patient’s level of pain, mobility, and any complications. Identify any related nursing diagnosis. |
| Management | Promote healing and prevent complications | Administer pain medication as prescribed and implement non-pharmacological pain management techniques. Immobilize the fracture site as appropriate and provide instructions for proper positioning and weight bearing. Provide patient education on the fracture, care and management at home, and expected time frame for healing. | Monitor the patient’s pain level, mobility, and wound healing. Provide patient education on the fracture, care and management at home, and the expected time frame for healing. Provide feedback to the healthcare provider as needed. |
| Evaluation | Monitor for complications and evaluate the healing progress | Assess for signs of infection, bleeding, or delayed healing. Monitor for any adverse effects from medications. Evaluate the patient’s adherence to the treatment plan and make any necessary adjustments. Monitor for any changes in the patient’s condition and adjust the care plan as needed. Reassess the patient’s need for continued immobilization. | Assess the patient’s progress toward healing and mobility. Document any complications or changes in the patient’s condition, and adjust the care plan as needed. Reassess the patient’s need for continued immobilization. Document the patient’s progress and discharge plan. |
Craniotomy The Treatment of head injury
RUHS BSc Nursing Entrance Exam 2019